If you’ve been told your options are limited due to talus damage or avascular necrosis, new 3D-printed solutions may offer a different path, one focused on preserving movement and improving quality of life.
For some of the hardest problems in foot and ankle surgery, patients used to face bad options and worse options. That is not hyperbole. It is reality.
When bone dies, when the talus collapses, when arthritis advances, when trauma destroys anatomy, the old reconstructive ladder often narrows quickly. Live with pain. Undergo a fusion with major tradeoffs. Accept stiffness, gait compromise, or a future that feels smaller than the one you had before. In the most devastating cases, even amputation becomes part of the treatment vocabulary.
Additive technology has changed that conversation.
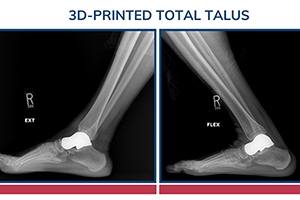
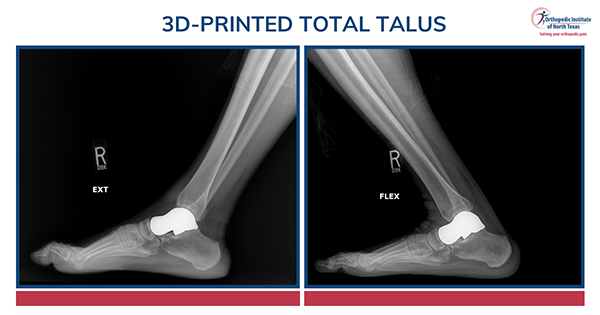
I am talking specifically about patient-specific 3D-printed solutions in foot and ankle surgery, especially 3D-printed total talus replacement, custom reconstruction for avascular necrosis of the talus, segmental bone loss, and highly complex limb-salvage problems. This is one of the most important advances I have seen in modern foot and ankle surgery.
But it needs to be said clearly: the value is not in the printer alone. The value is in how wisely the technology is used. This is not science fiction. It is not magic. And it is not a shiny toy. It is a powerful tool that can dramatically improve options for the right patient when it is paired with the right judgment, the right design, and the right surgical plan.
The first time I realized what additive technology could mean for foot and ankle surgery.
The first time this really hit me was during fellowship.
We had a young woman in her late teens who had been in a catastrophic motor vehicle accident and sustained a talus fracture. She went on to develop avascular necrosis of the talus with debilitating arthritis. At the time, we had heard reports out of Asia about total talus reconstruction, but it was not truly available to us here.
She was stuck.
Her options were terrible. She could live with severe pain and dysfunction, or she could undergo a fusion procedure with a relatively high-risk profile and no guarantees. Even if that worked, she would be fused with a TTC construct and spend the rest of her life living with rigidity, altered gait mechanics, and the downstream burden that comes with it. I pushed hard to see if there was any path toward compassionate use. There wasn't. We had no option to offer her that truly fit the problem.
That case stayed with me because it made me feel helpless.
Then in 2020, I saw the same problem again, but this time I was the attending. A young patient came to me after surgery elsewhere. His deltoid artery to the talus had been compromised, and he had developed avascular necrosis. He had no meaningful arthritis in the tibia or the calcaneus. It was, in many ways, a wash-rinse-repeat of the patient I had cared for in fellowship.
But now the technology was real.
We had a long, honest conversation. I told him this was not standard of care. I told him it was not FDA approved in the way patients often assume medical devices are. I also told him that his other options were poor, and that this might allow us to delay a much more morbid salvage procedure without burning future bridges. He was an engineer and very much understood the logic of a patient-specific solution.
That case was the turning point for me. It was the moment when additive technology went from a frustratingly unavailable idea to a real tool that could help a real patient.
Why the total talus changed everything
The foot is unlike any other part of the body.
It has 28 bones, 32 joints, and an astonishing level of complexity. We do not just need the foot and ankle to look acceptable on an X-ray. We need them to carry us through life. We need them to absorb force, transfer load, create motion, maintain balance, and tolerate the repetitive demands of walking. The mechanical burden on this anatomy is extraordinary.
Historically, when these problems became catastrophic enough, the old saying was essentially: fix it, fuse it, or lose it. That is crude language, but it reflects a real surgical truth. Once enough bone was gone or enough joint destruction had occurred, the solutions often became increasingly destructive in order to achieve stability.
The total talus changed that.
For me, total talus was the proof of concept. It was the moment I realized additive technology could move us from generic salvage toward elegant, patient-specific reconstruction. AVN of the talus is one of the most dreaded problems in foot and ankle surgery. It is dead bone in one of the most mechanically important structures in the lower extremity. Once the talus collapses, the clock starts ticking toward pain, loss of function, and degenerative arthritis.
For the first time, we had a way to address that problem in a manner designed for the specific patient in front of us.
That is a big deal.
What 3D printing actually means in foot and ankle surgery
Patients often hear '3D printing' and think one of two things: either it sounds futuristic and amazing, or it sounds experimental and scary.
It is neither.
This is not science fiction. Medicine has used versions of additive technology in other fields for a long time. Oral surgery, maxillofacial reconstruction, and dentistry have been using these concepts for years. Dentists literally do versions of this in their offices. The difference is that foot and ankle surgery is much more mechanically demanding. People do not walk on their teeth.
What additive technology allows us to do in foot and ankle surgery is create highly specific, patient-matched solutions to highly specific structural problems. In the case of a 3D-printed total talus, we can use advanced imaging and CAD modeling to design an implant that closely reproduces the patient's anatomy. We can restore shape, preserve limb length, correct deformity, and replicate the relationship between the ankle and hindfoot far more faithfully than traditional salvage procedures ever could.
That is why this is so compelling. Historically, many salvage procedures required us to sacrifice anatomy in order to save the limb. A patient-specific total talus does not do that in the same way. It is designed to preserve motion, preserve length, and allow the foot and ankle to move in a way that more closely mirrors how that person's anatomy was intended to function.
That does not mean it makes someone normal. It does not. As one of my mentors used to say, surgeons do not make people perfect. They make people different. But in the right patient, this can be a very meaningful difference.
Who is and is not a candidate for 3D-printed total talus and additive reconstruction
One of the biggest misconceptions in this space is that the pathology alone determines whether someone is a candidate.
It doesn't.
It is not just the X-ray. It is not just the MRI. It is not just whether there is AVN, bone loss, arthritis, or deformity. The candidate is the patient.
These are salvage-level reconstructions in many cases. Patients need to understand what they are signing up for. They need to be comfortable with a thoughtful surgeon-team collaboration. They need to understand that the goals are real, but also that the goals are not magical. They need to be ready to weigh realistic expectations, future revision possibilities, and the fact that these procedures are often chosen because the alternatives are substantially worse.
Technically, additive solutions can be applied to a broad range of pathology. But not every patient should be indicated for a total talus simply because it can be done.
Poor candidates include patients with unrealistic expectations, poor soft tissue envelope, and, for me, smokers in any non-urgent or non-emergent situation. Infection is not necessarily a deadend, but it usually changes the pathway into a staged reconstructive strategy rather than a straightforward implant case.
The right patient understands that this is not about chasing technology. It is about using technology to preserve function when the conventional pathway is grim.
What patients need to understand about avascular necrosis of the talus
AVN is dead bone.
I had this exact conversation with a patient recently. This is not 'partially dead.' It is not the movie The Princess Bride. Once the talus loses viability and begins to collapse, the ankle and hindfoot are often on a timer. Pain escalates. Arthritis advances. Function declines.
That is what makes AVN of the talus such a dreaded problem.
Historically, if AVN progressed far enough, the traditional salvage solution was often fusion, sometimes with bulk allograft. Those procedures can work, but they carry real morbidity and real complication risk. And if they fail, the next step is often far uglier. In many cases, you are running out of runway.
This is where total talus and additive reconstruction matter so much. They preserve motion. They preserve options. And importantly, they keep us on the playing field.
That phrase matters to me. One of the things I talk to patients about before we even fabricate an implant is the long game. For isolated total talus cases, I often frame five years as a baseline, not because the implant necessarily fails at five years, but because I want patients thinking in terms of future planning. If needed, we can revise to a combined total talus and total ankle construct. Technology is evolving quickly. The fact that we have preserved motion and preserved options means we are not at the end of the road.
Revision is not an afterthought in this field. It is part of the strategy.
Where additive technology fits in ankle arthritis, ankle replacement, and ankle fracture care
Patients with ankle arthritis often come in asking whether a 3D-printed talus is the answer.
Usually, it is not.
That distinction is important. Additive technology is primarily a way to address bone defects, bone loss, avascular necrosis, and structural failure. It does not replace the role of total ankle replacement. If a patient has ankle arthritis without talar collapse or major bone compromise, the conversation is usually about traditional reconstructive principles: fusion versus replacement.
Ankle arthritis is very different from hip and knee arthritis. Most ankle arthritis is post-traumatic. Our patients are often younger. They have higher demands. And the joint itself is more complex than many people realize. This is not simply a ball-and-socket joint or a straightforward hinge. It is a sophisticated mechanical system. We know ankle arthritis can be profoundly disabling.
That is why the modern treatment paradigm is shifting. We still debate fusion versus replacement in some cases, but there is no question that ankle replacement has improved significantly with better technology and better longevity. Additive technology becomes important when arthritis coexists with nonviable bone, bone defects, or talar failure. That is when combined constructs like total talus plus total ankle become highly relevant.
The same logic shows up in ankle fracture care, especially the bad fractures. Patients often assume a fracture is fixed once the bone heals. That is not always true. Fixing bone and fixing a damaged joint are not the same thing. Cartilage injury can set off a cascade toward post-traumatic arthritis regardless of how well the fracture was reduced. Severe fractures, talar injuries, and post-traumatic collapse are often what eventually lead patients into this reconstructive territory.
Why the real operation starts in the design session
One of the biggest traps in additive technology is thinking the technology solves the problem for you.
It doesn't.
The implant only executes the plan you bring to it.
For me, the design process is highly choreographed. Once we have the imaging, the CAD session becomes the operation before the operation. I meet with engineers, walk through the design, specify exactly what I want, review the mockups, and then refine the details until the implant reflects the actual surgical plan. Then I sign off.
That matters because engineers are incredibly talented, but there is a real difference between something that is engineer-led and something that is surgeon-led. The bridge between what can be designed and what will work in a living patient cannot be overstated. I can often tell immediately in other implant designs whether something was driven primarily by engineering logic or by surgical logic.
Surgeons go into every operation with a plan. Choosing the right plan is just as important as executing it. In additive reconstruction, that principle becomes even more important. Once the implant is built, that is what you have. There is no meaningful on-the-fly redesign in the operating room. If the design session was wrong, the implant will faithfully reproduce the wrong idea.
That is why this field is so intellectually demanding. The learning curve is less about manual difficulty and more about problem-solving. The technology is almost limitless in design potential. The limiting factor is whether the surgeon can identify the real problem, choose the right solution, and create something that is biomechanically sound, feasible to implant, and durable enough to serve the patient well.
What recovery, pain relief, and motion can look like after total talus reconstruction
One of the most surprising things for many patients is that recovery is often easier than they anticipated.
That does not diminish the seriousness of the surgery. This is still major reconstruction. There is still healing. There is still swelling. There is still rehabilitation. And patients still have to put in the work to get better.
But compared with the historical salvage alternatives, the recovery is often much more manageable.
For a straightforward isolated total talus, patients are often walking in a cast by one week after surgery, and many are in a shoe by around six weeks. Again, that is not a promise. It is a general framework. But it is an important one, because many of the alternative operations in this space are more morbid and more disabling.
What patients tend to value most is simple: standing no longer hurts the same way, and motion is preserved.
Range of motion is often maintained at least to the level patients had before surgery, but now the arc of motion is much less painful. I love the first postoperative visit for exactly this reason. When I gently range a patient's ankle and watch their expression change from nervous anticipation to visible relief, that is one of the most gratifying moments in practice. You can see them realize, in real time, that moving the ankle no longer brings the same pain.
That matters.
What also surprises patients is how emotional these outcomes can be. Many of these patients have spent a long time living in uncertainty, pain, and fear. They have been told versions of bad news. They have been cornered into poor choices. So when they regain function and stop thinking about the ankle every minute of the day, the gratitude is real. I have had patients cry out of relief and tell me they feel like the surgery saved their life.
Even the small moments are memorable. Before surgery, I often show example implants in the office. Patients are usually shocked by how heavy cobalt feels in the hand. They always ask whether they will notice that heaviness in the body. The answer is no.
Why surgeon experience matters so much in this field right now
This field is growing. The body of evidence is expanding. The playbook is being written in real time.
That is good news.
It also means that, right now, experience still matters tremendously.
I do not believe that will always be true to the same extent. Over time, as more surgeons gain experience, more data matures, and the reconstructive pathways become more standardized, the barrier between high-volume and low-volume users will likely narrow. But for now, surgeons who are deeply versed in this technology hold a distinct advantage in patient selection, implant design, trap recognition, and downstream planning.
That matters because the biggest risk in an expanding field is not lack of imagination. It is lack of restraint.
I worry about buzz. I worry about shiny new toys. Any expansion of new technology has to be done judiciously. Unfettered utilization opens the door to poor indications, unnecessary procedures, and poor patient outcomes. That is not a technology problem. It is a judgment problem.
Patients should not want a surgeon who sees every problem as an excuse to use a custom implant. They should want a surgeon who understands the full spectrum of options. In my practice, there is a strong emphasis on limb salvage. I have done the historical procedures. I do the modern procedures. I understand the pearls and pitfalls of both. That is why additive technology is valuable to me. It is not a hammer. It is a tool in a much larger bag, and my job is knowing when to use it and when not to.
What the future of additive technology in foot and ankle surgery looks like
The future is here, but it must be used wisely.
That is the core truth of this field.
Over the next five to ten years, I expect broader solutions, better technology, more standardization, and more availability. Patients should not have to travel across the country or across the globe to access thoughtful additive reconstruction. As the technology matures, it will continue to reshape more than just bone loss. Deformity correction, custom segmental reconstruction, revision support, and increasingly sophisticated solutions across foot and ankle surgery will continue to emerge.
And the exciting part is not simply that we can print implants. It is that we can do it in a way that is patient-specific.
That is the future: not generic salvage, but thoughtfully designed solutions tailored to the anatomy, biomechanics, and goals of the person in front of us.
At the same time, we need to be honest about evidence and uncertainty. There is enough real-world data to know that this works. This is not theoretical. But like any motion-preserving reconstruction, revision remains part of the conversation, and long-term data is still evolving. That means decision-making has to remain collaborative. Surgeon and patient have to weigh the opportunity, the limitations, the alternatives, and the unknowns together.
That is what wise use looks like.
What patients should know when looking for a surgeon for total talus or complex limb salvage
If you are searching for options because you have talar AVN, ankle arthritis with bone loss, a failed prior surgery, or a complex limb-salvage problem, my advice is simple: do not choose your surgeon based on the phrase '3D printing' alone.
Choose someone who understands all of the options, not just the newest one.
Choose someone who understands when additive technology fits and when it does not.
Choose someone who leads the design process rather than outsourcing the thinking.
Choose someone who can explain the plan, the recovery, the revision pathway, and the long-term strategy in a way
that makes sense. Choose someone who respects both the possibility and the limitations of the technology.
The right surgeon should make you feel two things at once: hope and clarity.
For a long time, many of these patients had bad options and worse options. Additive technology has changed that. It has created new pathways for preserving motion, maintaining function, and keeping future options open in cases that once felt boxed in.
That is why I believe so strongly in it.
Not because it is futuristic.
Not because it is flashy.
Because for the right patient, it can be life-changing.
And that is exactly why it must be used wisely.

Justin Kane, M.D.
Foot & Ankle Orthopedic Surgeon
Dr. Justin M. Kane is a board-certified, fellowship-trained orthopedic surgeon specializing in foot and ankle surgery at the Orthopedic Institute of North Texas. He focuses on both advanced reconstructive procedures and minimally invasive techniques, treating complex conditions such as deformity, trauma, arthritis, and limb salvage cases. Dr. Kane has a particular interest in patient-specific solutions, including 3D-printed reconstruction, and is committed to helping patients preserve motion, restore function, and return to an active lifestyle through thoughtful, individualized care.